Hasn't the NPA got it Wright?
P3 Pharmacy,
12 Oct 2021![]() 5 Min
5 Min
P3 Pharmacy,
12 Oct 2021![]() 5 Min
5 Min
P3 Pharmacy,
12 Oct 2021![]() 5 Min
5 Min
The Review Steering Group looking at the future representation of community pharmacy in England continues to take soundings, but has yet to provide concrete options for change. Rob Darracott says there’s much to like in the position and outline proposals developed by the NPA over last 18 months
In its latest (August 2021) update, the Review Steering Group (RSG) tasked with considering the 33 recommendations of the Independent Review of Community Pharmacy Contractor Representation and Support (the ‘Wright Review’) says so far it has been focused on engaging with the sector. It is now reflecting on feedback from engagement sessions over the summer and is refining “new models for representation and support – setting out the ‘how’”.
The National Pharmacy Association (NPA) is focused, first and foremost, on the ‘what’. It says pharmacy tends towards a focus on the price of things, rather than the value in getting things right. A good outcome for its members would be “a system that is more effective, not only more efficient”.
“Fundamentally, we need an enabling funding settlement, constructive relationships and integrated planning that combine to sustain the development and implementation of clinical services over the long term,” the NPA says. There’s a lot to unpack in this statement, but including the development of community pharmacy’s clinical services and capacity is itself significant.
investment in skills and leadership development at all levels could have transformational and enduring benefits
Contrast that with the RSG’s expected benefits. It too wants representation to “operate more effectively”. But “it should also mean that we reduce duplication between national and local organisations and that everyone’s focus is directed onto high value activities that best support contractors. The changes should also lead to more standardisation, meaning consistency of representation and support services for contractors across the country.” I don’t know what that means to a community pharmacy contractor busy keeping the show on the road.
The RSG says it is now “developing options for models (my italics) of future representation and support”, focusing initially on the functions of the national and local representative bodies. It is also working on how contractors will agree on proposed changes, probably early in 2022.
As well as negotiating the contractual arrangements for England as a whole, the RSG “believes a strong national body could” set a direction for community pharmacy, improve negotiating outcomes, have a stronger voice and provide better support to local organisations.
Inter alia, negotiating local contracts and services is included in an overarching statement of what the RSG wants local representative bodies to be doing, but not the list of functions. There is a reference to integrated care systems (ICSs), but the function will be to “respond to local consultations”.
The NPA has developed its thinking over time. In January 2020 its contribution to the Wright Review set out ’10 Guiding Principles’ for what it wanted as “outcomes for the profession and our members” (see box). These principles contain key proposals, notably for a national service development unit, which made it into the review report. The NPA says now: “We believe these remain wholly pertinent and, if realised, represent a joined up whole sector outcome.”
The NPA’s current position anticipates the impact of ICSs. Although this was partly a timing issue, a major criticism of the Wright Review was its lack of recognition of how the direction of travel for the NHS might impact the needs of community pharmacy representation.
Asked what principles the review should be guided by now, the NPA says: “Community pharmacy needs more support at a local level. The NHS has begun to move decisively in the direction of commissioning for population health needs at a local level. It would be sensible to consider in depth how investment in skills and leadership development at all levels could have transformational and enduring benefits.”
This has to be the right approach, and is one likely to be endorsed by local leaders, who are faced with calculating where they can have the most impact in arguing for pharmacy input to new integrated care pathways. The NPA recognises, much more clearly than the RSG, that both national and local plays are required. It says: “We should move forward on the basis of achieving an end-to-end representation structure capable of influencing at the national contracting level and the point of deployment and delivery at the coal face.
“The opportunities in driving growth in emerging ICS local commissioning could well bring us fresh service roles and revenue growth more easily than the national contract has in recent times.” With ICSs due to be in place from April next year, this is also urgent.
Speaking to me on 29 September, NPA chief executive Mark Lyonette said: “My concern is how quickly the world is moving round us. I’ve sat in meetings with the NHS and the Department of Health where they’ve felt enabled to tell us we are moving too slowly. I have a lot of sympathy when you’re dealing with structures changing all the time, but that’s not a reason to not do anything. If we’re not moving quick enough to deal with the challenges of the day, we’re disadvantaging ourselves further.”
“Service development should be primarily based on local population health needs and delivered through integrated local care pathways,” the NPA said in response to questions. “Local integration can only be achieved by having an optimised structure of strong local representation that builds trust and influence over time. It is self-evident that the task of embedding community-centred ways of working can only be delivered with strong local input.”
Recommending increasing the capacity for local service development last year, the NPA said: “Local is where the magic happens; it’s where ideas are conceived, innovation is sewn and patient care is delivered. Local capacity for effective support and representation is especially important in the light of the funding (£4.6 billion) for primary care via primary care networks. Public Health England has clearly signalled that community pharmacists must engage with local authorities, the voluntary sector and other local stakeholders, as partners in whole-systems care.”
More than ever, we need great local leadership – that’s largely relationship building
It’s hard to see how any of this can be delivered if community pharmacy engagement locally is directed nationally. Central Health’s recent success [link to come] is a case in point.
The NPA is also the only organisation so far to articulate what the future representation of the sector might comprise. In a paper produced in the middle of 2020, the Association published its ‘Changing the Model’ diagram (below). “The right support needs to be given at the right level, in order to avoid duplication and release resources both locally and nationally.”
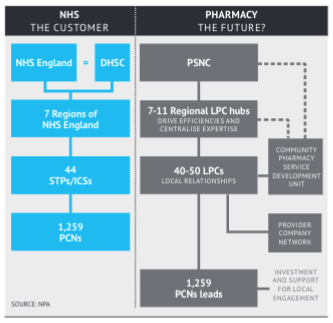 Rather than concentrate local support functions at the centre, the NPA proposed a number of “regional LPC hubs” to drive efficiencies and concentrate expertise. “This could release money (by further reducing duplication of mechanical administrative spend) for reinvestment in local representation,” it said. The service development unit is there too “to coordinate the development of ideas bubbling up from LPCs via regional hubs.”
Rather than concentrate local support functions at the centre, the NPA proposed a number of “regional LPC hubs” to drive efficiencies and concentrate expertise. “This could release money (by further reducing duplication of mechanical administrative spend) for reinvestment in local representation,” it said. The service development unit is there too “to coordinate the development of ideas bubbling up from LPCs via regional hubs.”
“I’m very conscious of how the balance of national and local is changing,” Mark Lyonette says. “More than ever, we need great local leadership – that’s largely relationship building. When I talk to LPCs, you can see those that have invested the time over the years; they are now sitting quite well and are capable of seeing where they fit into an ICS landscape. Those that haven’t are the ones saying we need the NHS to impose places on ICS boards. That’s not going to happen, nor will it solve the problem if it did.”
‘Changing the Model’ also recognises the role of provider companies, a welcome recognition of those out there making progress. Significantly, the NPA suggests this might be a “provider company network”, rather than a national provider company. Not being prescriptive seems sensible at this stage; provider companies, where they exist elsewhere in primary care (optometry, GP Federations have some similar functions), they have developed organically.
This ‘starter for 10’ for a future structure appears to have received little attention so far. It’s certainly not had a public response, which is a pity. The RSG’s most recent engagement events have discussed the functions that might be delivered at a national or local level, but an initial suggestion for the structure of a multiagency ‘contractor support system’ could help narrow the options.
“Local, national (and possibly also regional) structures of representation and support should be connected and integrated; meaningful flow of insight and learning between PCN leads, LPCs, regional hubs and community pharmacy sector central teams would ensure that all parts of the system benefit one another. Much of what ultimately emerges in the national contract originates from local innovation supported by LPCs.”
David Wright and his team spent months taking views before recommending the need for “system-wide change”. The NPA has accepted the premise, and envisaging how that might look will bring it to life for many. As a trade association with voluntary membership, the NPA’s input needs to be recognised as the views of its members, not just as a single contribution to the debate. As a trade body veteran in a number of sectors, Mr Lyonette says: “The reason our members belong to us is for us to do some of that work for them. It’s not legitimate, in a sector like ours, to say you must turn up to a contractor forum and express your views. It’s critical contractors take the final decision, but the reason they pay their dues to bodies like us is for those bodies to represent them.”
As of September 2021, the NPA’s concerns with the possible outcomes from the RSG’s work and the proposals that may emerge are several. Importantly, given the focus in this article on where the future lies (we will look at the NPA’s suggestions for getting contractors’ consent to changes in a future article), the NPA says: “The current RSG proposals imply a significant disinvestment in local support beyond efficiency gains from streamlining the network (of LPCs). There is no clear plan to recognise the shift within NHS decision-making and maximise the community pharmacy influence on the new local NHS structures (both ICSs and PCNs).”
The NPA is unhappy that there is no business case yet for new or expanded functions in the national body, or indeed any financial modelling setting out the allocation of funding across the future structures, whatever they may be. It is also unclear where control of the money would sit in future – effectively, control currently sits with LPCs. It would be hardly a surprise to find an expanded PSNC arguing that it should also allocate the money; given the absence of a clear rationale for where functions might sit – another reason the NPA’s outline model is helpful – there is more danger of reaching the wrong conclusion.
The NPA’s final concern on the current list, however, is that “there is no plan to define what ‘good looks like’ for a contractor in terms of what they get for their levy investment into PSNC and LPCs; and there is no mechanism to deliver performance across the structures”. Which is where we started.
The RSG has promised to put some meat on the bones of its work soon. It is hard to envisage that this will not be options for structural change, but if ‘options for models’ is what we get, the NPA’s considered contribution to the discussion to date bears further scrutiny. If nothing else, it might help contractors think about ‘what good might look like’. And demand it.