An LPC redesign for our times
P3 Pharmacy,
15 Nov 2019![]() 2 Min
2 Min
P3 Pharmacy,
15 Nov 2019![]() 2 Min
2 Min
P3 Pharmacy,
15 Nov 2019![]() 2 Min
2 Min
 By Aneet Kapoor
By Aneet KapoorCommunity pharmacy in Greater Manchester has had a turbulent few years. The announcement of a devolved health and social care budget in 2015 enabled GM pharmacy leaders to start to negotiate enhanced opportunities for community pharmacy contractors to better support the health system. Devolution prompted a merger of six of the seven LPCs in GM in 2016, and the formation of CHL, the community pharmacy provider company.
Opportunities to reduce duplication, leverage efficiencies of scale and further expose community pharmacy’s role in the health and wellbeing of the GM population were maximised by a new committee and employed team who quickly built relationships with key stakeholders across GM. However, a fragmented approach to commissioning by ten localities with varying priorities, financial pressures and views of community pharmacy has made it challenging to carve out the additional locally commissioned service opportunities predicted at the outset.
Since 2016 work has been done to standardise community pharmacy services across GM, with the inhaler technique and minor ailments services being frontrunners and commissioned by multiple localities. A smoking cessation service is under development and a novel commissioning model is in the final stages of sign off, which will allow the harmonisation of service specifications across GM, and a single GM contract for community pharmacy with a standard IT platform for data collection, reporting and payment.
The rate of change of the NHS landscape has been unprecedented and 2019 has proven to be a pivotal year for community pharmacy in England. The advent of primary care networks, the NHS Long Term Plan and a five-year funding deal for community pharmacy have led to a compelling need to review and adapt to better support the new skills and guidance pharmacy contractors require in the emerging NHS landscape. In January, GMLPC initiated a piece of work to review its infrastructure in order to enhance business performance, and to respond to the needs of new business priorities.
A deep dive into the operating model the LPC was undertaken with the whole team and supported by organisational design consultants. That review suggested the organisation would benefit from re-structuring its workforce around business reform resulting from a shifting external market place; particularly, to optimise organisational resource capacity and capability while continuing to build a robust centralised corporate function for stability.
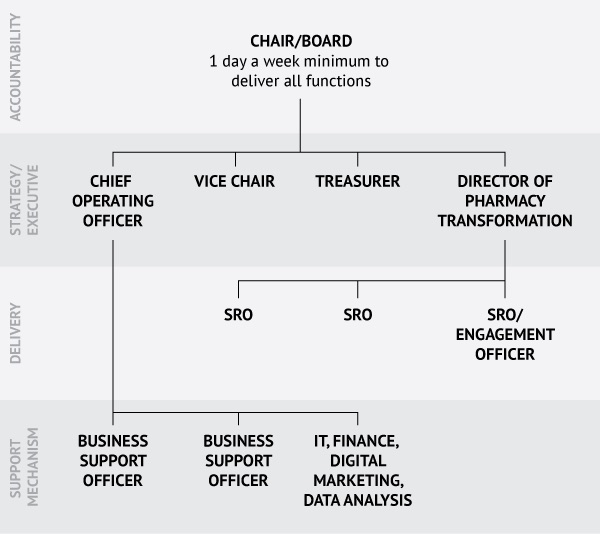
The creation of internal and external facing executive roles was agreed to close the gap between strategy and delivery. Current operational delivery roles were streamlined into thematic senior responsible officer (SRO) roles to align human resources and business workstreams, stimulate a self-managing, high performing team and embed industry-based expertise into both ‘business as usual’ and growth activity. A need to further develop the maturity of HR, IT, finance and business intelligence and administration functions to accommodate the stability of core internal business functions was also identified and built in to the restructure.
LPC Committee members roles were transitioned from locality leads into ‘champion roles’ to enable the skills and expertise of GM’s pharmacy experts to operate beyond traditional boundaries, and also work to mentor and upskill the workforce at the frontline to lead. Underpinning the changes are clearly defined and articulated role profiles from board to front line delivery, and an organisational structure which was agreed to be fit for purpose for the foreseeable future.
The new intended structure of the LPC is notably led by a director of pharmacy transformation (DoPT); a crucial role in ensuring the role outlined for pharmacy in the Long Term Plan is realised within the five year deal period. The need for sound leadership in tune with the changing landscape is key for community pharmacy, and it is imperative their sole focus is on the delivery of this transformation.
The role of the chief operating officer is just as crucial to relieve the DoPT of much of the LPC administrative burden previous chief officers have, while the thematic SRO roles provide expertise within each domain of our strategy and business plan and are the enablers for successful delivery. The DoPT will be the point where SROs covering Primary Care Networks (PCN), Services, Engagement and our Greater Manchester Healthcare Academy come together to deliver for community pharmacy. PCN integration is key for community pharmacy and is where potential service opportunities will arise. If and when these opportunities arise it is key for all of community pharmacy to be engaged and upskilled as a team in order to deliver. You can see how the roles are key.
The newly formed role descriptions focus on outputs and key metrics to demonstrate value for money. They are supported by a structure which has clear accountability and responsibility to help drive operational efficiency and create the necessary expertise to support contractors through the changing landscape. Existing roles within the office team were mapped over, creating opportunities we have gone out to market with.