
In Interviews
Follow this topic
Bookmark
Record learning outcomes

Tariq Muhammad has his mojo back. Five years after the demise of Pharmacy Plus, the firm he founded and developed into a national provider of pharmacy services to care homes, his technology company Invatech Health will be demonstrating its Titan PMR pharmacy platform at the Pharmacy Show with full NHS approval.
“The technology is just the means to an end,” he says. “I’m not here to sell PMRs – yes I am, I’m a business at the end of the day – but that isn’t the purpose. The purpose is what’s wrong with your job, and what’s wrong with what people are experiencing. Let me show you how I use technology to join this together in a road map for the future.”
Tariq qualified as a pharmacist in 1992 and completed his pre-registration year at Southmead Hospital, a teaching hospital in Bristol. “It was very clinical,” he recalls. “You’re thrust into ward rounds, drug information, your brain cells being used on a daily basis. That was what I thought pharmacy was going to be.”
While he loved the environment, he was not a fan of the system. “I think I have something of my father in me; I couldn’t really see myself working up a ladder,” he says. Without a day’s experience in community pharmacy, that’s where he headed. “I remember my first customer. The assistant said, ‘this patient wants to see a pharmacist’. I thought this is my chance to shine. The person asked me to change a camera film. I missed a lot of lectures at university… It was almost at that moment, on the first day, that I realised what I had gotten into, and I didn’t like what I saw.”
Although in the hospital he would change prescriptions that were not pharmaceutically correct, when he queried GPs’ prescribing, he was shouted at. “I was this close to jacking it in, do business, accountancy. But I decided to stay and do it my way.”
I went to the PMR companies for a system that could give me head office control, data, reporting. They all looked at me funny
After 18 months failing to get a new pharmacy contract, Tariq made an offer for a rundown pharmacy he worked in as a locum. To buy it, he sold his car and took out a loan. He relocated the pharmacy to a more prominent site down the road, designed the new premises himself; three consulting rooms; a training room for patients. Pharmacy Plus opened in January 1995. As Bedminster Pharmacy it’s still there. Tariq sold it to Ade Williams.
“I ripped out the cosmetics. I wanted the pharmacist to be on show. I created a workflow with two pharmacists – I would be in the consulting room, we’d sit patients down, write little chits, make our own extemporaneous products. That pharmacy went from 1,000 to 10,000 scripts a month in a year. People would come in for prescriptions, advice, medicines, disability aids. I had a model.”
More pharmacies followed. He moved to a head office. By 2000, Pharmacy Plus was 20 pharmacies across the southwest, from Plymouth to Gloucester. The challenge then became a different one. “My model worked well in high volume areas, but unless you were getting prescriptions you couldn’t do anything else. So, as much as I hated it, I found myself in retail, otherwise I wouldn’t have had a business.”
Other hard lessons followed. “The name on the door doesn’t make any difference, it’s down to the quality of the pharmacist. Dosette boxes, nursing homes, deliveries were a distraction from the main business of dealing with people.” Growth also inevitably meant losing the tight control over a business that can be exercised over a smaller number of outlets.
After looking for solutions, he started writing software in 1999
 That was the spur to look to technology for solutions. “I went to the PMR companies for a system that could give me head office control, data, reporting. They all looked at me funny.” He started writing his own software in 1999 for his head office warehouse function. It worked. “It fixed the buying; I added staff management, training manuals. Then I decided pharmacists were doing a lot of stuff they didn’t need to do, like home delivery – why are you doing that in a shop with a £25k rent, when you could do it in a shed? Nursing homes, the same.”
That was the spur to look to technology for solutions. “I went to the PMR companies for a system that could give me head office control, data, reporting. They all looked at me funny.” He started writing his own software in 1999 for his head office warehouse function. It worked. “It fixed the buying; I added staff management, training manuals. Then I decided pharmacists were doing a lot of stuff they didn’t need to do, like home delivery – why are you doing that in a shop with a £25k rent, when you could do it in a shed? Nursing homes, the same.”
Tariq says he thinks he was the first to create a hub and spoke operation, centralising nursing home dispensing, dosettes and home delivery, using his own software centrally and “leaving good pharmacists to do great services” in his branches. When he saw more potential centrally, he sold most of the pharmacies, and set his sights nationally. He stopped coding himself, and his new programmers developed his original CAPA (consolidated application for pharmacy administration) system, with the aim of eliminating dispensing errors.
“It made me think very differently, because the onus was on me. It led me, in 2004/5, into barcoding. Printing labels and going to look for stock is not foolproof. I decided to print something that says, ‘go and bring me the stock’. If I scan it and it’s what I’m expecting, I’ll give you a label for it.” He found uses for scanners across processes. Claims for missing items led to bag labels only being produced once all products on a prescription had been scanned. Waiting three months to get a submitted prescription returned to deal with a query led to scanning prescriptions on receipt, and working from an image that would be retained to deal with any later arguments. Cameras were added to dispensing stations, MP4 files to records.
By 2006 Pharmacy Plus was barcoding, scanning at every stage, including its drivers scanning and barcoding bags into vans. Their building in the Bristol suburb of Eastville was like a mini-Amazon, conveyors everywhere. It was a pharmacy, an IT company, a logistics business.
Nursing homes were next in line for a fix. “We were really slick, but a nurse would give the drug to the wrong patient in the nursing home. And they’d look to blame us. I thought until I can fix the nursing home problems my business isn’t safe, so in 2006 I extended the barcode journey with the first eMAR (electronic medication administration record) in the UK. I’d seen laptops on trolleys in America, but they’d converted paper to screen. But it wasn’t about the screen, it was the barcode.
“This was the holy grail – I could see everything. I knew everything about the patient, what they took, when they spat the drug out. I could see a doctor prescribing 100mg sertraline, but the patient has been spitting out their 50mg for the last month. He doesn’t know what’s happening, but I could start making a clinical difference.”
A career long motivation to innovate
He returns time and again to the motivation to innovate. “The destination has never changed from the day I qualified. I don’t like what I see in pharmacy. I feel let down that the profession hasn’t done something sooner. I’ve had my ups and downs, and I’ve demonstrated that you can create new models of pharmacy practice – hub and spoke, centralisation. We held the record for the largest monthly volume until Pharmacy2U took us over a couple of years ago.
“But it was never about being the first, it’s just these things are necessary. I want the pharmacist’s role to be intervening in medicines supply based on evidence. Supply is our responsibility and we have to do it safely and efficiently. When we were doing 250,000 prescription items a month all of my pharmacists were on clinical services.”
His story arrives at the elephant in the room. The collapse of Pharmacy Plus. I ask what happened. He says: “From 1994 to the end I owned 100 per cent of Pharmacy Plus. I didn’t answer to anyone. Sure, we had day to day challenges like any other business - banks, stocks, suppliers. I even had pharmacists charging me £50 a hour in the fallow year. But never once did I not enjoy coming to work. People joined because they enjoyed the ride; they believed where we were going.
“In 2012, Pharmacy Plus was third in nursing home business behind Boots and Lloyds. I was presented with a unique opportunity to provide services to one of the largest care home chains in the UK. Fantastic.
“We worked on a plan to scale up for six months, and at the last minute they told us our balance sheet wasn’t strong enough. I was given a choice – scrap the deal, or accept a solution, a venture capital investor, who would take a minority shareholding. Gut told me no, but head said, ‘what is there not to like?’ So I took on a minority shareholding from a private equity company in order to fulfil a large contract. My problem was that my customer and my investor were the same.”
Tariq says that within three months a Category M cut and Aricept coming off patent wiped a million pounds off the company’s earnings. “We go into underperformance. One year after the anniversary of the investment, these guys have control of the business. They sack my finance director, everyone – guys who’ve been with me for 20 years. I’m by myself.
“I now comply, or leave. For the first time in my life I don’t want to come to work. In the Autumn of 2013, I leave my own business, hand my resignation to the investors and I go home.” Tariq says the investors who’d hoped to buy his shares at a fraction of the cost were disappointed when the business was assessed as inherently valuable. Money was put in, but Pharmacy Plus was haemorrhaging customers. They decide to put it into administration in May 2014. Tariq says: “People will say ‘why should I trust this guy?’ But in 20 years in business, I’ve never not paid a supplier or failed to serve a customer. I took on investment, the pharmacy remuneration model is not designed for specialist operations and the investors didn’t know how to run this type of business. It was horrible experience to see what I had created destroyed, but a big lesson was learnt.”
The comeback was swift. A month after Pharmacy Plus went into administration, Tariq set up Invatech Health. “I bought the IP [intellectual property] from the administrators, got my people back together. We were on a journey. We recognised that we were trying to do too much. The clever bit was the IT, because we understood processes.
“We used to be the bad boys, taking business away from people. So rather than be the enemy we decided to be the supporter of pharmacy. First thing off the ground was a lighter version of CAPA for pharmacy, and we rewrote the software for the care home system, which we rebranded as Atlas. We were back in business with a different model.”
Reaching for the moon
The model went into Wales in 2015 thanks to a Welsh Government grant and a partnership with Cardiff University; a joint venture with Well, who sold Atlas into their care home customers, followed. “It was around 2016 when I decided the real need was to build a new PMR,” Tariq says. “The PMR is the epicentre of the pharmacy operation, and because of the NHS EPS accreditation, there’s been no innovation. It’s the same system I had in my shops, nothing has changed. EPS has put a barrier down, so anyone new has to go through this huge process.”
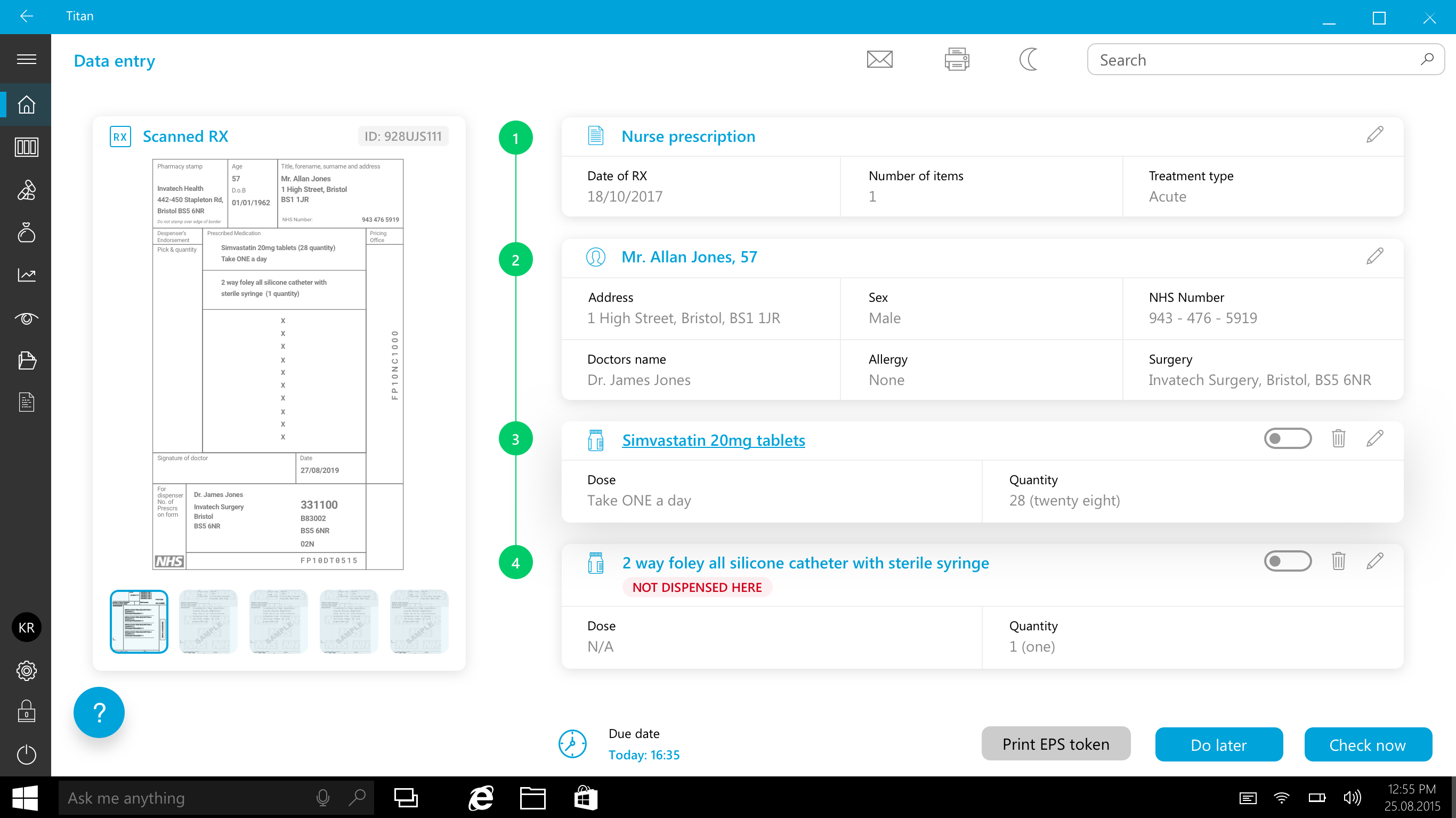
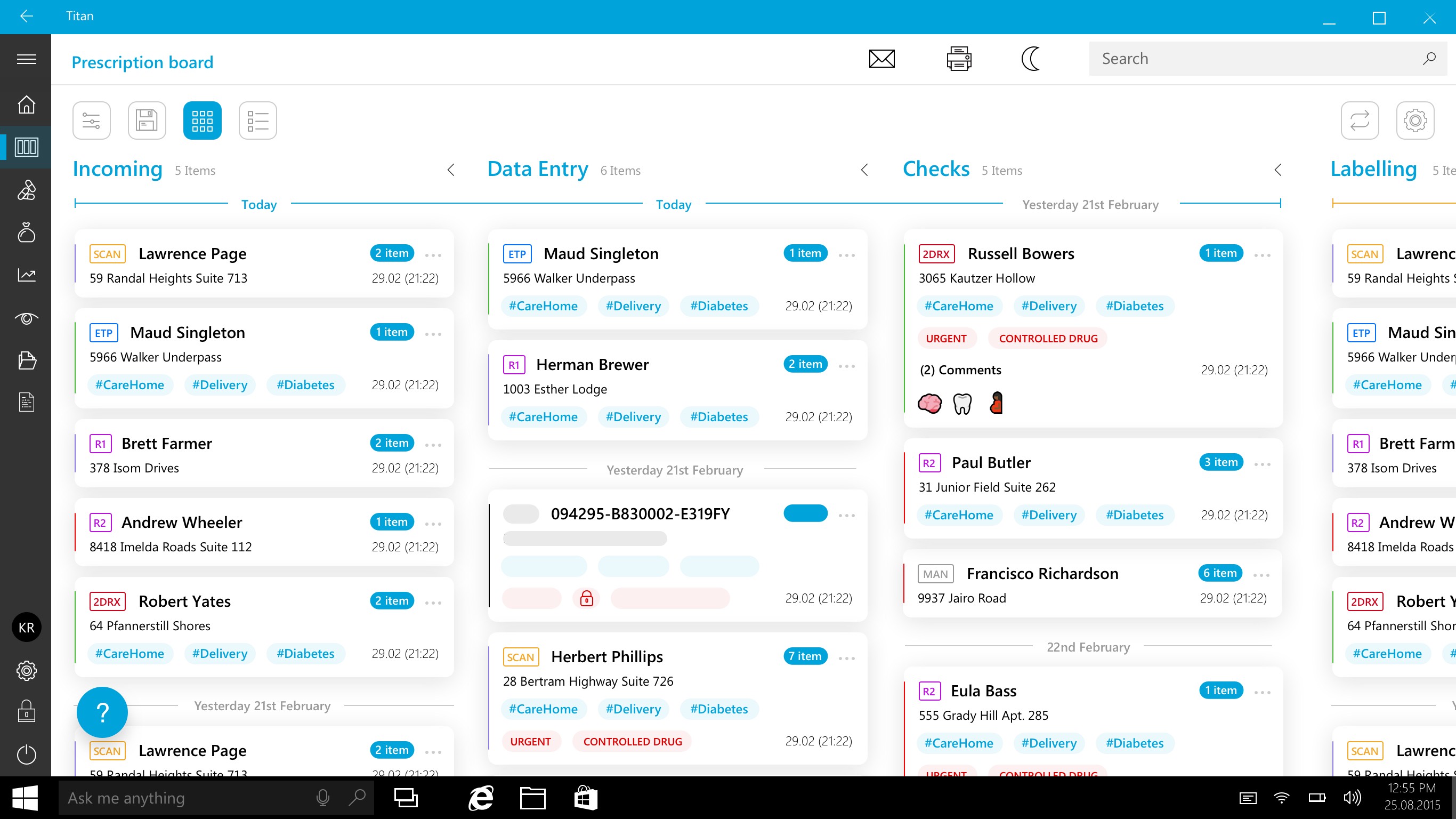 Titan reinvents the PMR by visualising the dispensing process workflow and scanning at every stage to improve safety
Titan reinvents the PMR by visualising the dispensing process workflow and scanning at every stage to improve safety
He chose to build from scratch. Tariq says. “It would have been easier to take a legacy system. We decided to build a modern system with new technology, but with all the hindsight of 25 years.”
So, paper prescriptions become images, barcodes are added. Patients can follow the progress of their prescription on a large screen, like in Argos. Prescriptions appear on the system’s dashboard, in priority order like an inbox. Progress through the dispensing process is via Kanban board, which depicts the work to be done at various stages. Everything is touch screen.
Print picking label. Scan. Print product label. Scan dispensed labels on products into bag. Print bag label. Scan bag, screen tells patient it’s ready. Scan patient ticket as final check (or scan text message when patient comes to collect). Send claim automatically; FMD. A scan.
 There’s more. “We can create APIs [program interfaces] through the cloud for plug in apps. It might be you have a robot, or an MUR program. It’s like we’ve created the iPhone. We own what it comes with, but what makes your iPhone unique is the apps you put on it. We’ve really created a platform, but if we didn’t call it a PMR people would ask us what it is.”
There’s more. “We can create APIs [program interfaces] through the cloud for plug in apps. It might be you have a robot, or an MUR program. It’s like we’ve created the iPhone. We own what it comes with, but what makes your iPhone unique is the apps you put on it. We’ve really created a platform, but if we didn’t call it a PMR people would ask us what it is.”
We’re talking a couple of weeks after Titan’s accreditation for EPS came through at the end of an 18 month process. Around a hundred independents are using CAPA as a pharmacy back office to a care home using Atlas. “Our aim is to enable independents to grow with a more efficient business,” Tariq says. “Titan integrated with CAPA will help pharmacies grow their prescription volume and become profitable through better workflow.” He says he also has several tenders for supplying Titan to chains on his desk – “they were waiting for our accreditation”.
It's the difference between having a bicycle and a rocket to go to the moon. We’ve got the rocket, and it’s fuelled up.
“The end goal is to achieve real change in pharmacy. To get pharmacists out of the dispensary, to carve out the future as we should have done 20 years ago. If you understand the back story you can see why I’m still here. It may sound corny, but every day, we are one inch closer to the destination.
 “Old systems were built in a paper world. When EPS came in, the option chosen was the easiest – print the token. NHS Digital needs to deliver paperless. This is the difference between having a bicycle and a rocket to go to the moon. We’ve got the rocket, and it’s fuelled up. And our customers are not dependent on us for the next feature. You can customise Titan like people choose toppings on pizza.”
“Old systems were built in a paper world. When EPS came in, the option chosen was the easiest – print the token. NHS Digital needs to deliver paperless. This is the difference between having a bicycle and a rocket to go to the moon. We’ve got the rocket, and it’s fuelled up. And our customers are not dependent on us for the next feature. You can customise Titan like people choose toppings on pizza.”
Tariq thinks his biggest problem will be compliance with a system built on scanning, not paper. “People need to go through a change process. We are saying ‘there is no prescription’. They might have two terminals now for 15,000 items, because all they are using their computer for is printing the token and reams of labels. We come along and say you need five.
“Pharmacy is sitting on a very weak foundation. Years of under investment in technology. If all pharmacies had barcode scanners, FMD would cost nothing. We did FMD in five minutes, because we were already scanning a 1D barcode. Everyone was scratching their heads because they want the exemption check at handout. We coded in the check in 15 minutes.
“Henry Ford said that if you ask people what they want, they say faster horses. If you ask pharmacists what they want, they say put this in the top corner and my labels will come out faster. Pharmacists need someone who has felt the pain, and knows what prescription they need.
“I’ve been on the other end. The group of people who have been with me since 1999 are still here. We’ve been to the end of the earth, nearly died, but if you want to get there, we’ll tell you how. How to change the patient experience, how to change your experience. You need to stop doing this job here, and you need to be over there doing that job, because that is your future. Here’s your life raft. That’s what Titan is.”