Focus pharmacists on core to improve efficiency
P3 Pharmacy,
05 Sep 2019![]() 4 Min
4 Min
P3 Pharmacy,
05 Sep 2019![]() 4 Min
4 Min
P3 Pharmacy,
05 Sep 2019![]() 4 Min
4 Min
Whichever way you want to look at it, the national community pharmacy agreements across the UK are predicated on assumptions that community pharmacy can be more efficient to create the headroom for more (and different) clinical services. Operational improvement specialist Andy Chilton of Velresco says there’s plenty of capacity to be released by taking a detailed look at your existing processes
“There is a very clear window of opportunity to capitalise on freeing up capacity, not just to stave off the impact of cuts to item payments, but to get ready to deal comfortably with new service requirements and develop new public and private services,” Andy Chilton says. “But pharmacists can only delegate their current tasks if the team have the capacity in terms of safety and quality. We know that can be done. We have the evidence. On average, halving what we actually observe and being conservative in our calculations, there are 50 hours a month per pharmacist, and that is delegable because we have found 67 hours per month, on average, in the dispensary process and elsewhere. That’s 10 million hours to the system, to the sector, of available service delivery time…almost for free.
“We are so confident we can find a three to one return on investment in hours equivalents, that if we can’t, we will give you the money back.”
Mr Chilton says operational improvement specialists like Velresco find opportunities to release capacity by making things work more effectively. “Largely that’s about identifying, quantifying and removing non-value adding activities, or finding things that could be done differently.”
Leadership, team dynamics, skills and capabilities are all in scope. Velresco has completed more than 150 studies in community pharmacies – looking at layout, flow and movement of work, and the equipment being used and how things vary, even when those carrying out the work aren’t aware of that variation. “We look at the quality of the equipment, is it fit for purpose? Can it be found when someone wants it? It’s not unusual to find six hours a month attributable to not finding equipment where it’s meant to be.”
“Some of it’s dead easy to get at,” he says. “For example, if somebody comes in to collect something, you could waste two, three minutes, each time, trying to find their script if you don’t ask ‘is it due yet?’ There is no point hunting for a script that ain’t there. We freed up over 15 hours per month in one multiple’s dispensaries just by getting staff to ask a few key questions to avoid that unnecessary hunting.”
We are so confident we can find a three to one return on investment in hours equivalents, that if we can’t, we will give you the money back
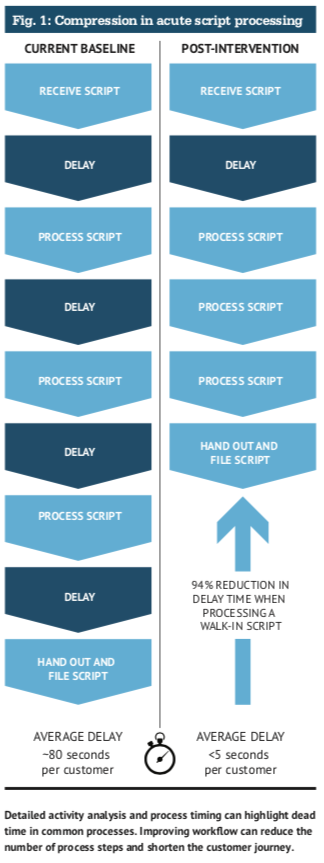
He says Velresco helped another client move from an average of 12 minutes per acute prescription to five, within a day of implementation. “If you keep an acute script patient in store, you avoid adding steps to the process at the back end. There are four extra steps if you encourage someone to pick up later. This is not about working harder, or faster, but by doing less of what doesn’t add value, by doing things slightly differently or better, or possibly even substituting an activity (Figure 1). This might be through automation, but there is so much you can do in many cases before having to consider a robot.
“Importantly, if you can reallocate some of the tasks people carry out under a walk in to just the dispensary team, the pharmacist could be freed up to have an MUR conversation and the customer is getting pure added value. And it becomes a wait-free experience from their point of view.”
 That change certainly resonates with Velresco customer Fin McCaul, of Prestwich Pharmacy in Bury. He says the amount of time a prescription is ‘dead’ was an eye opener. “It’s in a basket waiting for a check, or bagged and waiting to be handed out. Your priority might be waiting scripts, but you have as much dead time as actual process time,” he says. “Once the team were able to see the outcomes from making changes, they were ‘yes, please, let’s get on with it’.”
That change certainly resonates with Velresco customer Fin McCaul, of Prestwich Pharmacy in Bury. He says the amount of time a prescription is ‘dead’ was an eye opener. “It’s in a basket waiting for a check, or bagged and waiting to be handed out. Your priority might be waiting scripts, but you have as much dead time as actual process time,” he says. “Once the team were able to see the outcomes from making changes, they were ‘yes, please, let’s get on with it’.”
Like many in the field, Velresco maps processes, gathers timing data and creates improvement programmes by assessing the value of different activities. Velresco divide activities (Table 1) into those that are:
Core – add pure value
Enabling – indirectly add value, is important to completing a task, but needs to be minimised or delegated to someone else, or
Inhibitive – do not add value, because they do not need to be done at all, they are wasted effort.
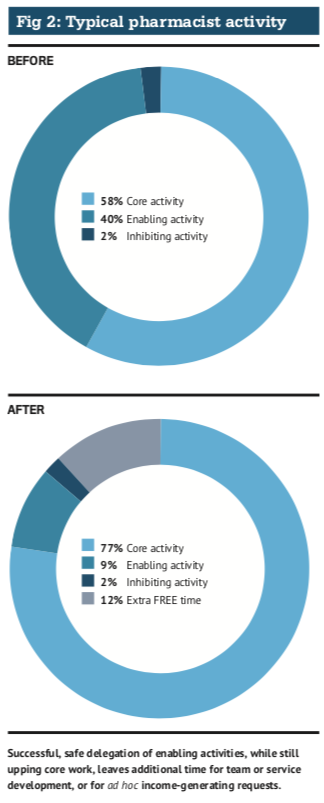
“The pharmacist should only be doing those core things nobody else is qualified to do,” says Mr Chilton. “In fact they should have spare capacity, particularly for what’s coming down the line with the new Community Pharmacist Consultation Service (CPCS), which represents an ad hoc requirement for their time. They can only capitalise on that opportunity if they’re delegating away the enabling activities, and reducing or eradicating the inhibiting ones.” Figure 2 shows a typical pharmacist activity allocation before and after a Velresco intervention.
Velresco says its service takes half the time of traditional studies, which halves the costs too – a typical single site Velresco study will cost around £6,750. Velresco’s trademarked v-Flow software simplifies data capture (via tablet, picture, top) and performs an initial analysis “It also makes studies better, because we can keep our heads up looking for things, and listening to conversations,” says Andy Chilton. “We find three times as many opportunities compared to manual methods. If you like, we’ve become much more productive at leveraging productivity.”
Typical Velresco studies include three types of assessment:
Day in the life role-based activity studies
Whole system examination to achieve more throughput
Process activity timing to calculate how many people in which role are actually needed.
“v-Flow allows us to analyse instantly, so we can engage with the pharmacist and the team there and then, starting the journey of change. If we can show the evidence, it’s difficult to refute. A very rapid journey is not just about acceptance of the evidence, but ‘what can we do differently’?”
Table 1: Types of task |
|
| Core activities | Routine activities that only the current pharmacist role should perform, but these can be done in a different way |
| Enabling activities | Routine activities that the pharmacist role needs to perform to complete core activities, but can be simplified and/or delegated |
| Inhibiting activities | Ad hoc interruptions or disruptions to the pharmacist workflows that can be reduced or removed |
Improvement studies start with a half day briefing visit, used to build trust with the pharmacy team and calibrate the v-Flow tool to the pharmacy. “It typically takes an hour or two for people to stop noticing you. We need to be invisible, on the edge, looking in.” Observations on common processes start the next time the team go in. “We don’t just look at what’s happening and how, we try to establish why it’s happening this way, so we can understand the cause and think about how we can make it different. We give staff an opportunity to tell us things, or we might ask for clarification; it’s very inobtrusive.”
We freed up over 15 hours a month in one multiple’s dispensaries by getting staff to ask a few key questions to avoid that unnecessary hunting
A further day of process observations will follow, although with a purposeful gap. “We then find that people are comfortable to come to us with their ideas.” Velresco’s ideas capture tool VWall is used to harvest thoughts on how things could be improved. “It helps to justify change to management if their own team is asking for it.”
The third full day of observation is used for the ‘pharmacist day in the life’, after which Velresco produce a report, which is presented verbally and discussed over half a day with the management team or the pharmacy owner. A simulation exercise is used to get teams ready for what good looks like. “It’s fun but challenging,” Mr Chilton says. “It prepares people for the investment in time or money required to make change happen and stick, so when we present the findings to them there’s no resistance. They’re ready for the next stage, which is experimentation and solution design.”
Julie Horslen was part of a National Pharmacy Association (NPA) trial of Velresco’s approach three years ago, before she sold her Prestwood Pharmacy in Buckinghamshire. “The staff really enjoyed reading their report because we were a ‘high functioning, dispensary team’. We did work well together, but Velresco suggested that, as good as that was, dispensary staff should take a bit of a back step; they were helping counter staff too much.
 “Velresco also analysed our MDS boxes operation and we realised just how much time and effort it was for the money. As a result, I told the staff not to get upset with losing an MDS box, as there were plenty of things to fill our time with. I think highlighting to staff how much time they were spending doing something not very cost-effective made them feel better.”
“Velresco also analysed our MDS boxes operation and we realised just how much time and effort it was for the money. As a result, I told the staff not to get upset with losing an MDS box, as there were plenty of things to fill our time with. I think highlighting to staff how much time they were spending doing something not very cost-effective made them feel better.”
Andy Chilton first came into pharmacy as a senior consultant at award winning boutique consultancy Boxwood after 19 years in the chemicals industry, most of them as an internal operational improvement consultant. The opportunity ultimately led to pharmacy being a key area of interest when Velresco was established in 2010. The company also works with vets, facilities management, retail and leisure, but pharmacy holds a continuing fascination.
“You can look at pharmacies in excellent form and there will still be opportunities,” he says. “We look at things second by second to hunt them out. The 80/20 rule applies. Some are easy to get at, others you might need to invest a little bit of money, for example, you might need a new counter to give you that extra bit of runway to get work to flow properly.” As to differences between independents and stores in a group, he says: “We’re probably going to find the same dozen or two key levers, but it’s a bit like a graphic equaliser; it will be applied differently in different places. In all cases, the team need to be owners of the solution, because then it will stick. the study plays a critical role in this.”
He cites storage of prescriptions awaiting collection as an example. “The best way we have found from a measurable, evidence point of view, is alphabetical, because you’ve got one movement. If you have a matrix system [with prescriptions stored alphabetically, annotated for location], there are two steps involved. You can save as much as 20 hours a month on that. It’s not just the pick-up, you have one step instead of two to put it away. It sounds like very little – you might save 20 seconds per script, but when you add that up…Some people initially say, ‘I’m not so sure about these cumulative small impacts making an effect’, but it works for Formula 1, so why not in pharmacy?”
For Fin McCaul, the Velresco study has continued to bring benefits. “You have to engage to understand what Velresco are doing,” he says. “But the biggest outcome for me is that we are now continually reviewing what we are doing; we haven’t stopped. Staff now ask, ‘why are we doing this’? ‘Why can’t we change that?’ Just yesterday, the team developed a new set of checklists of daily, weekly and monthly activities, with who has what job and who is responsible for specific areas.”